THE LIVANTA
CLAIMS REVIEW
ADVISOR
| |
A monthly publication to raise
awareness, share findings, and
provide guidance about Livanta’s
Claim Review Services
|
| Higher-Weighted DRG Review – Sampling Strategy | | Decreasing Medicare’s Paid Claims Error Rate | |
| |  |
A primary objective of the Medicare claim review services contract is to work toward decreasing Medicare’s paid claims error rate and protecting the Medicare Trust Fund. Livanta developed and implemented the Improper Payment Reduction Strategy (IPRS) as a tool to accomplish this important objective. The IPRS outlines the strategy Livanta uses to sample claims for short stay review (SSR). As a living document, Livanta updates the IPRS annually and incorporates empirical findings from reviews conducted during the previous year.
BFCC-QIO Authority to Conduct Claim Review
“The BFCC-QIO shall conduct ‘Short Stay Reviews’ per 42 CFR 412.3, 42 CFR 405.980, and Hospital Outpatient Regulations and Notices (OPPS) and inpatient prospective payment system (IPPS) rules including annual updates, revisions and amendments as published in the Federal Register. These reviews should be conducted on a sample of Medicare post-payment Part A claims for appropriateness of inpatient admission under the Agency’s Two Midnight Rule for acute care inpatient hospitals, long-term care hospitals, and inpatient psychiatric facilities.”[1]
Livanta devised a flexible approach to sampling that could accommodate monthly fluctuations in SSR claim volumes for potential selection and review, as outlined in Livanta’s IPRS, which was approved by the Centers for Medicare & Medicaid Services (CMS). The goal of this approach is to review short-stay claims in a manner that is more likely to uncover errors than would a purely random sample, while still being able to reconstruct justifiable regional and national improper payment amounts for all paid SSR claims. The second goal of claims review is to identify hospitals with high SSR error rates, educate hospital physicians and appropriate staff, and, if they are persistently non-complaint, refer them for further review as directed by CMS.
[1] FY 2016 OPPS Final Rule, CMS-1633-F, effective January 1, 2016.
| | SSR Sampling Strategy and Claims Weighting | |
As noted above, Livanta’s recently updated IPRS was informed by completed short-stay reviews. The prior year of completed reviews provides actual data to support evidence-based sampling. This approach applies the use of historical data to identify (1) diagnosis-related groups (DRGs) most likely to be paid in error and (2) providers with high denial rates. The details of the methodology are described below.
Sampling Prioritization Scores
Sample prioritization scoring is a statistical process approved by the CMS in which individual components of short stay claims are weighted. The resulting weights are grouped into sampling strata based on their estimated relative risk of improper payment. Higher priority strata are sampled at higher rates than lower priority strata. The ongoing review outcomes inform subsequent weighting and strata assignment.
Livanta’s flexible approach involves a compensatory prioritization system for targeted sampling. This strategy consists of three components: (1) volume-growth by CMS Certification Number (CCN); (2) clinical risk; and (3) length of stay (LOS). The findings from the second year of SSR reviews were published in the March 2024 Claims Review Advisor and can be found here: https://www.livantaqio.cms.gov/en/ClaimReview/files/The_Livanta_Claims_Review_Advisor_March_2024.pdf
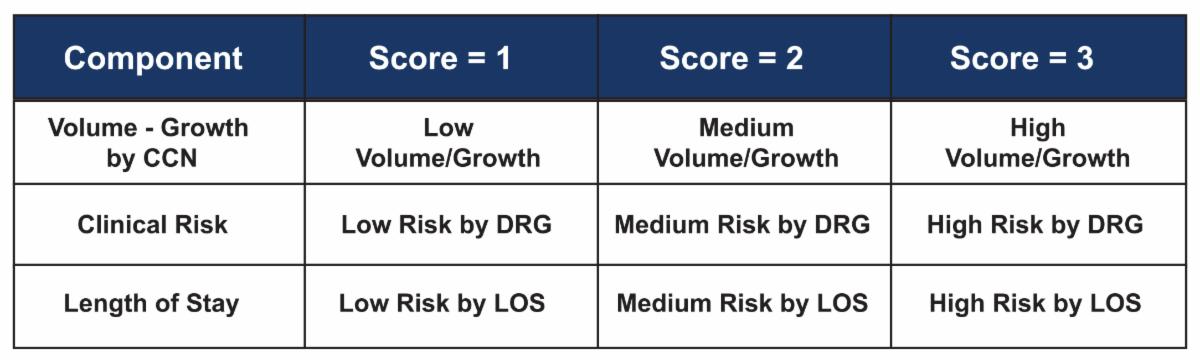
Livanta’s updated IPRS retains the compensatory prioritization system for selecting SSR claims likely to be in error, as shown in Table 1 below.
Table 1: SSR Compensatory Score
| |
Sampling Components
- Volume-Growth by CCN: Hospitals submitting the highest number of inpatient short stay claims and hospitals with the highest volume growth of short stay claims are prioritized.
- Clinical Risk: Analysis of the diagnosis related groups (DRGs) most often denied informs this category for ranking the DRGs as high, medium, or low risk of improper payment.
- Length of Stay: This risk component is informed by an analysis of length of stay (LOS) using both the inpatient admission date as well as the from date on the claim.
Sample and Extrapolation Adjustments
Unless the total listing of eligible claims (the population) is sufficiently large, there will be times when the allocated number of claims for each stratum will not be met by the number of claims that are eligible for sampling from the designated strata. Under those conditions, the additional claims are selected from the higher priority strata, in concert with the stated goals of the IPRS.
Technical denials are issued when a medical record has not been received for review in a timely manner. Although the subsequent submission of the needed documentation may reverse the technical denial, these denials can be avoided by submitting the supporting documentation upon request.
| | Individualized Hospital Results | |
When a hospital has had at least 30 claims sampled and reviewed over a rolling 3-month period, those claims are aggregated to form a hospital-specific report, which is then sent to the hospital. The report summarizes information the hospital has already received during the course of the monthly claims review process and includes identified areas for educational intervention where findings warrant.
The process of accruing monthly review results over time allows for identification of hospitals with higher error rates. Livanta selects targeted 30-claim provider samples each month to trend hospitals’ performance and tailor education, in line with CMS priorities for hospital education.
Livanta aggregates individual provider results and assesses educational opportunities at the provider level. Provider samples are analyzed, and one-on-one education is scheduled with a Livanta Medical Director and Coding Educator if a high error rate is noted.
| | What Can Hospitals Expect? | |
Hospitals can expect to receive medical record requests by fax or mail for sampled short stay claims at the beginning of each month. These sampled claims will be reviewed for the appropriateness of inpatient admission under Medicare’s Two-Midnight Rule. The greater the number of short stay claims that a hospital submits, the higher the likelihood that some of their claims will be sampled and reviewed.
These requests will be addressed to the medical record contact the hospital has designated in the Memorandum of Agreement (MOA) effectuated with Livanta. If a hospital has multiple claims sampled in a month, the medical record requests will be transmitted in one package.
| |
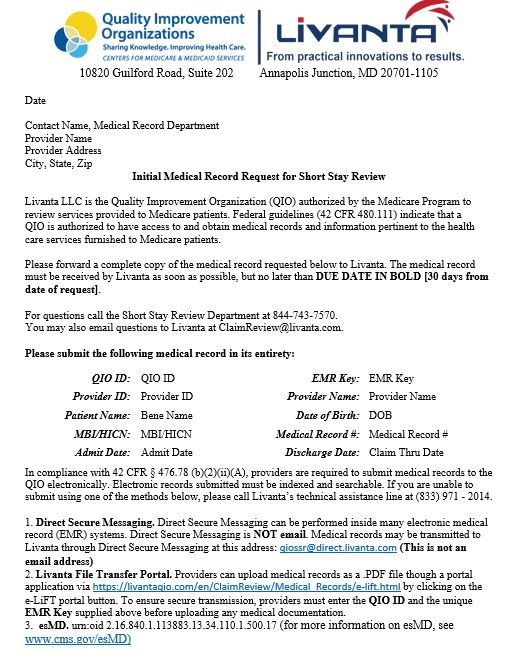
Figure 1: Example SSR Record Request | | Livanta is the Medicare Beneficiary and Family Centered Care-Quality Improvement Organization (BFCC-QIO) conducting post-pay fee-for-service claim reviews of acute care inpatient hospitals, long-term acute care hospitals, and inpatient psychiatric facilities to determine the appropriateness of Part A payment for short stay inpatient hospital claims. These claims are reviewed in accordance with the Two-Midnight Rule published in FY 2014 Hospital Inpatient Prospective Payment System (IPPS) Final Rule CMS-1599-F, as revised by CMS-1633-F. | |
ABOUT LIVANTA LLC AND THIS DOCUMENT - Disclaimer
This material was prepared by Livanta LLC, the Medicare Beneficiary and Family Centered Care - Quality Improvement Organization (BFCC-QIO) under national contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services. The contents presented do not necessarily reflect CMS policy and are intended for educational purposes only. 12-SOW-MD-2024-QIOBFCC-TO342
| | |