|
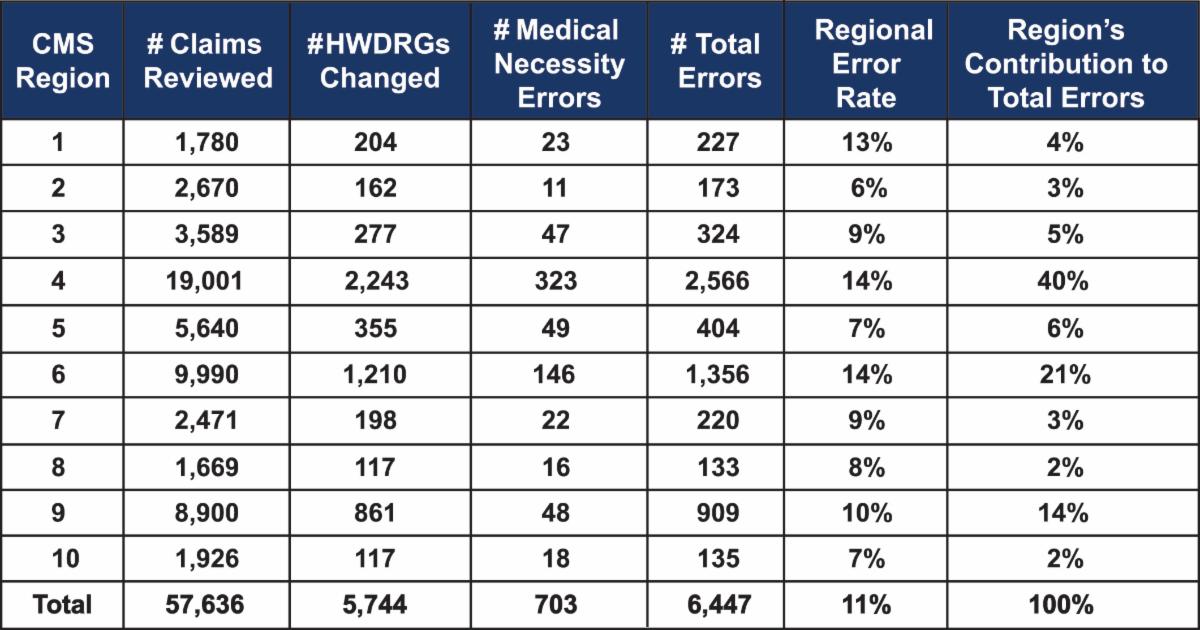
Region 1 - Boston
• Connecticut, Maine, Massachusetts, New Hampshire, Rhode Island, and Vermont
Region 2 - New York
• New Jersey, New York, Puerto Rico, and the U.S. Virgin Islands
Region 3 - Philadelphia
• Delaware, District of Columbia, Maryland, Pennsylvania, Virginia, and West Virginia
Region 4 - Atlanta
• Alabama, Florida, Georgia, Kentucky, Mississippi, North Carolina, South Carolina, and Tennessee
Region 5 - Chicago
• Illinois, Indiana, Michigan, Minnesota, Ohio, and Wisconsin
Region 6 - Dallas
• Arkansas, Louisiana, New Mexico, Oklahoma, and Texas
Region 7 - Kansas City
• Iowa, Kansas, Missouri, and Nebraska
Region 8 - Denver
• Colorado, Montana, North Dakota, South Dakota, Utah, and Wyoming
Region 9 - San Francisco
• Arizona, California, Hawaii, Nevada, American Samoa, Commonwealth of the Northern Mariana Islands, Federated States of Micronesia, Guam, Marshall Islands, and Republic of Palau
Region 10 - Seattle
• Alaska, Idaho, Oregon, and Washington
|