|
1. Congress Adjourned for 2023; What's Next for the 2024 Medicare Physician Payment Cuts?
2. Announcing PHA's Four New Board Members
3. HCA's "Grand Plans" - Blake Madden of Hospitalogy Takes a Look; 2024 PHA Leadership Summit Speaker
4. U.S. House Passed Site Neutral Payment Legislation Before Adjourning
5. What We're Reading: New Federal Government Merger Guidelines, New IDR Fee Rule & More
| |  | |
6. PHA's Summit Recap Available: Latest Legal Issues for PHA Members
7. PHA's Grassroots Campaign: Ask Your Patients & Employees to Engage Congress
8. Save the Date: PHA's 2024 Leadership Summit: September 21-23 at the Ritz Carlton in Naples, Florida
9. Thank You to PHA's 2024 Sponsors
| | |
Medicare
1. Congress Adjourned for 2023; What's Next for the 2024 Medicare Physician Payment Cuts?
| | |
Congress adjourned for 2023 without addressing the 2024 Medicare physician payment 3.37 percent cuts. This is partly due to the fact that Congress passed a continuing resolution in November that funds the federal government through early 2024. As a result, Congress did not have to address a year-end spending package, which incorporated Medicare payment cuts in past years.
What’s Next for 2024?
The 2024 payment cuts begin on January 1, 2024. Congress will need to address another funding package in January, and that package could incorporate some relief for the 2024 Medicare physician payment 3.37 percent cuts.
In the past, Congress addressed Medicare physician payment cuts in a retroactive manner.
Click here to view a December 13, 2023, letter from dozens of members of Congress urging Congressional leadership to fix the cut.
At this point, it’s difficult to address the scenarios, but some scenarios include:
- A complete reversal of the cuts. (Or even a slight increase.)
- A partial reversal of the cuts, such as what happened to the 2023 cuts.
- Congress does not address the issue.
What About a Permanent Fix?
The 2015 MACRA laws was supposed to replace the sustainable growth rate (SGR), which required an update almost every year, with a permanent solution to end Medicare payment cuts. However, it clearly did not solve the payment cuts.
Fast forward to today, and a growing number of members of Congress are calling on a new fix to address Medicare physician payment cuts. Because the upcoming year is an election year, it may be challenging to pass a major policy change. However, it is possible.
The GOP Doctors Caucus, which consists of the physicians and other clinicians in Congress, released draft legislative principles in October to create a new Medicare physician payment formula. Future Congressional legislation may incorporate the principles:
Section 2. Updating the Budget Neutrality Threshold
- Increasing budget neutrality threshold from $20 million to $53 million and increase every 5 years by the cumulative increase in Medicare Economic Index (MEI) since the last update to the threshold.The $20 million was established in 1992 and has not been updated since. This would allow for greater flexibility in determining pricing adjustments for services without triggering across-the-board cuts.
Section 3. Budget Neutrality Corrections for Overestimates and Underestimates in Utilization
- Provide a lookback period to reconcile overestimates and underestimates of pricing adjustments for individual services no later than 9/1 of the subsequent year. This would allow for the Medicare conversion factor to be calculated with more accuracy based on actual utilization data and claims.For example, if CMS proposes something for CY2025 that requires a budget neutrality adjustment based on projections of how much a new code or service was going to be utilized, data would then be collected on the accuracy of those projections, and CMS would propose a correction based on actual CY2025 utilization data for the CY2027 Physician Fee Schedule.
Section 4. Timely Updates to Direct Costs Used to Calculate Practice Expense RVUs
- Requires the Secretary to, no less than every 5 years, update prices and rates for direct cost inputs for practice expense (PE) relative value units (RVUs) which includes clinical wage rates, prices of medical supplies, and prices of equipment.CMS did not update supply and equipment prices from 2005-2019 and clinical staff wage rates from 2002-2022. The length between updates made price changes more significant rather than if prices were updated more frequently, which creates larger swings in payment than if more consistently updated.
Section 5. Limitation on Year-to-Year Conversion Factor Variance
- Starting in 2025, the Secretary would be required to limit positive or negative increases in the conversion factor to no greater than 2.5% each year. The policy goal is to provide stability for the PFS by removing relatively large and abrupt changes in conversion factor calculations.
| | |
PHA
2. Announcing PHA's Four New Board Members
| |
PHA's Board of Directors recently added four new directors:
Daniel Durrie, MD (Kansas City)
iOR Partners | Chairman of the Board
William Hotchkiss, MD (Dallas)
Carrell Clinic | OrthoLoneStar | North Central Surgical Hospital
Diane Hritz (Washington, Pennsylvania)
CEO, Advanced Surgical Hospital (Pennsylvania)
Mark Valentine (Dallas)
President | Baylor Scott & White The Heart Hospitals Enterprise Denton, Plano & McKinney | Co-leader, Cardiovascular Service Line, Baylor Scott & White Health
| |
Industry
3. "HCA's Grand Plans" - Blake Madden of Hospitalogy Takes a Deep Dive
| |
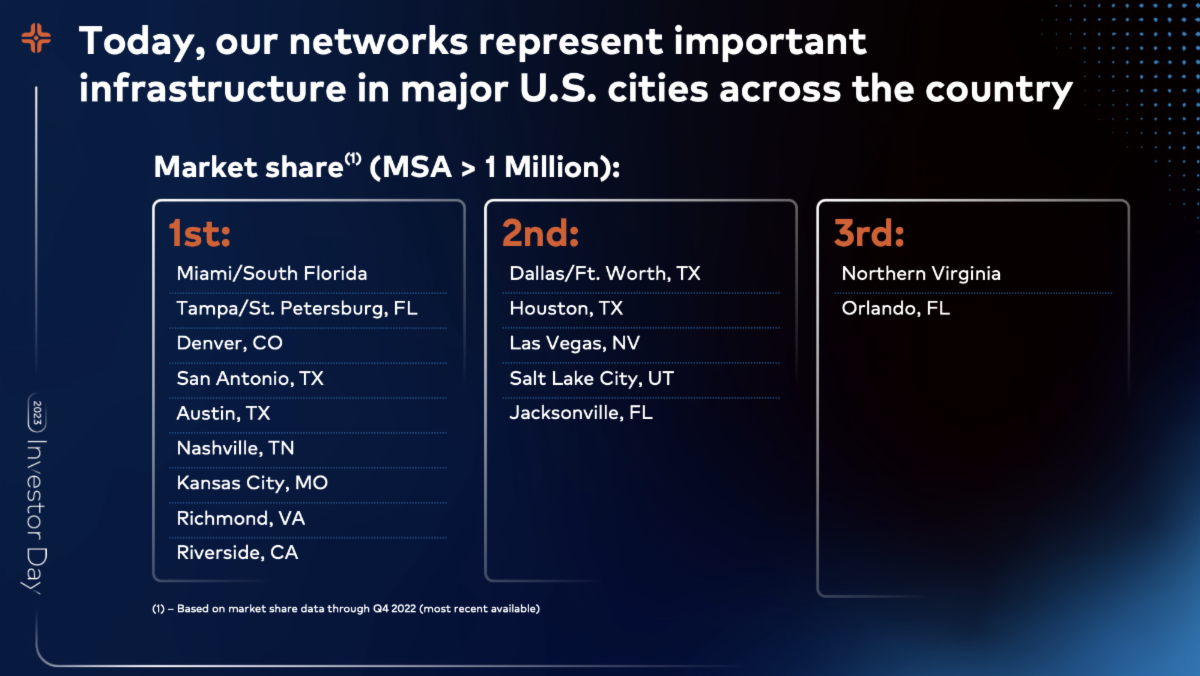
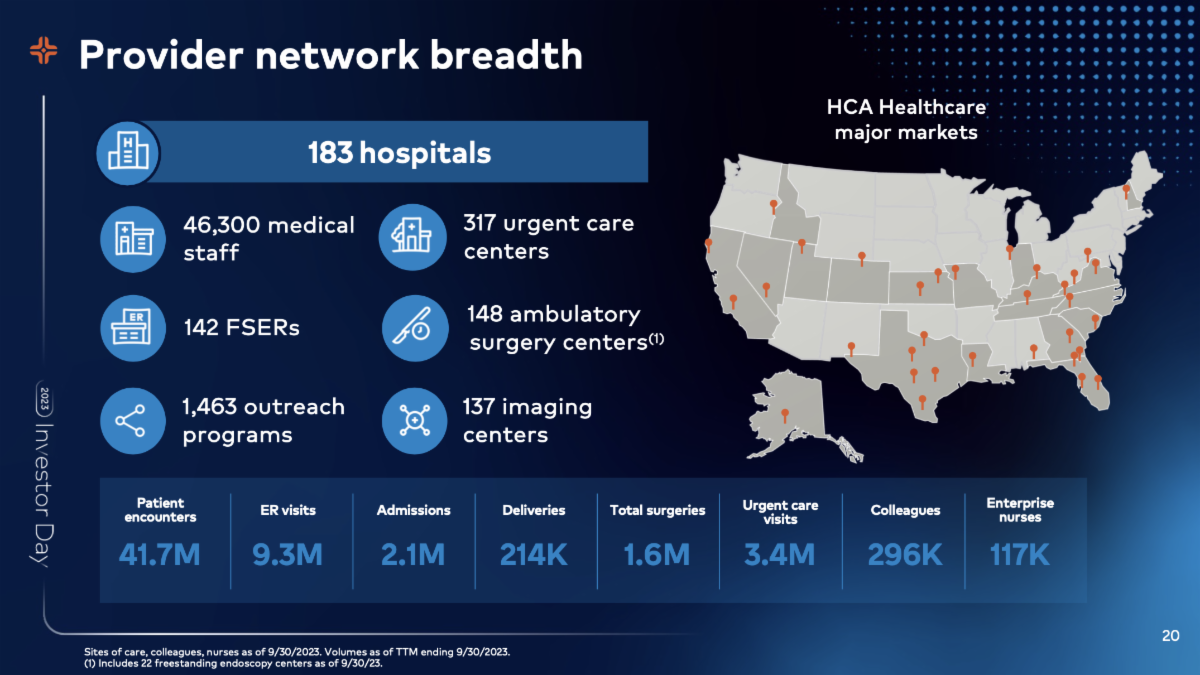
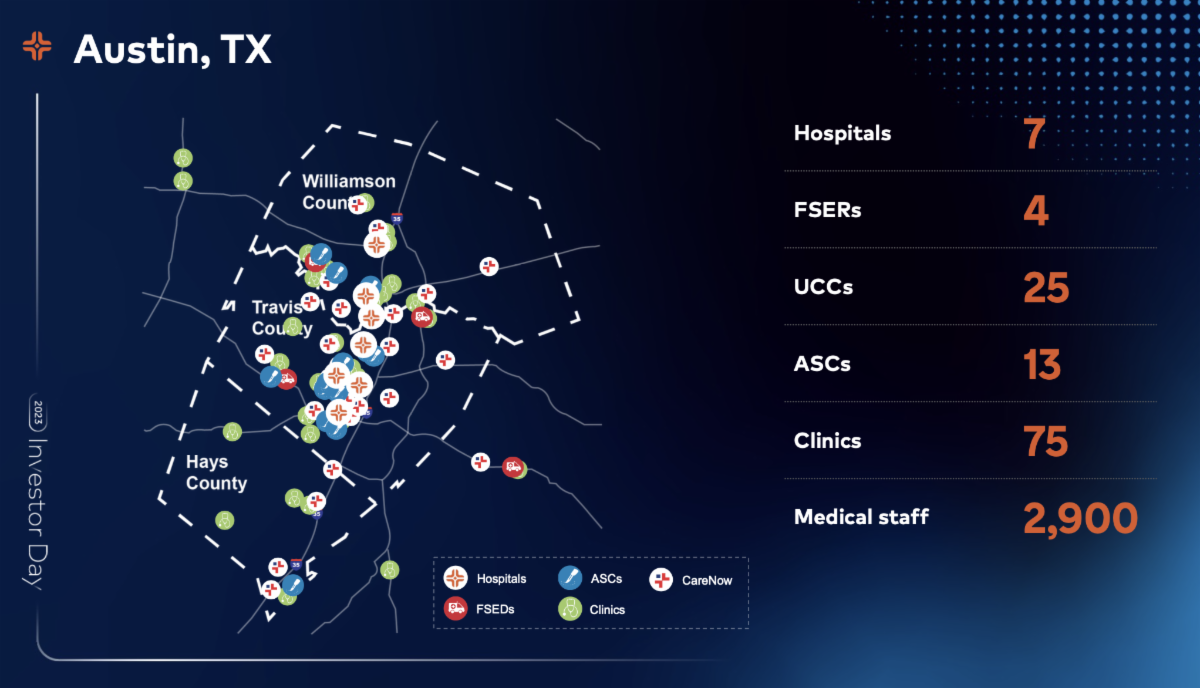
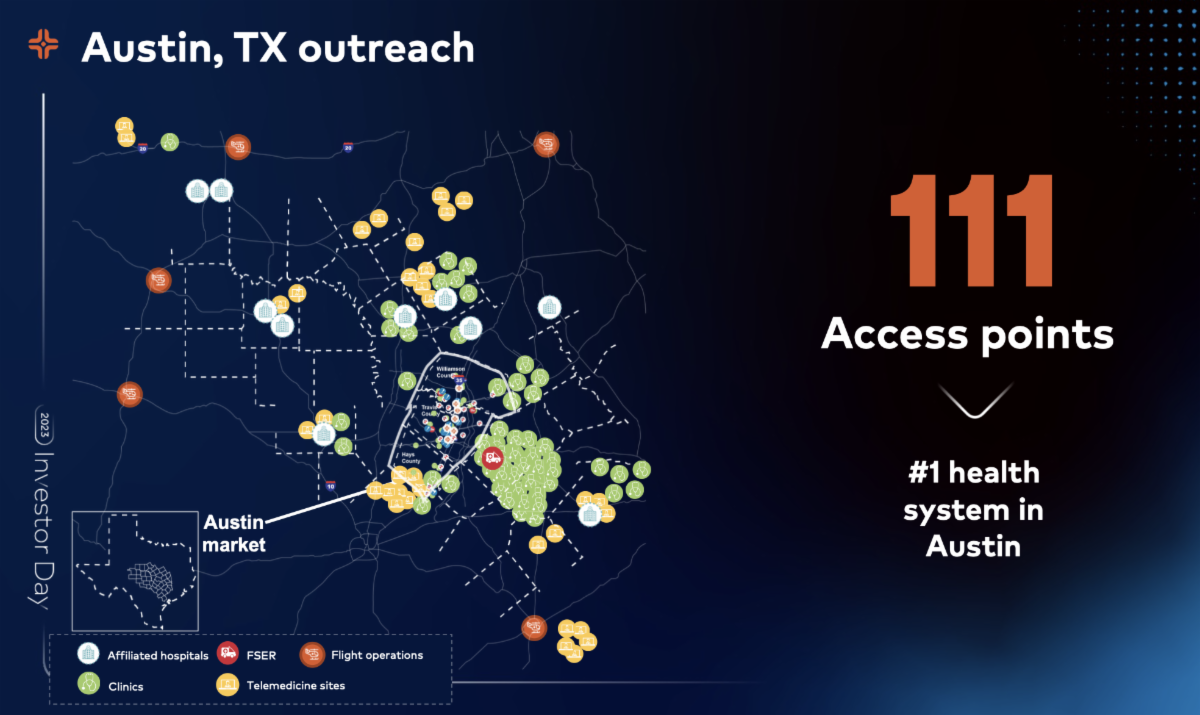
Blake Madden of Hospitalogy recently took a two-part deep dive into HCA's investor day. HCA announced a number of new moves in several markets, such as Florida and Texas, over the past few years.
Blake will be one of PHA's 2024 Leadership Summit speakers September 21-23 at the Ritz Carlton in Naples, Florida.
Blake's HCA Analysis
Click here to view Blake's full analysis. The slides at the bottom can be found in HCA's investor book in the link.
"HCA’s Success: It’s all about Markets and Density, Dummy"
In this section, Blake takes a look at HCA's success, despite threats over the years:
In its opening investor day remarks, HCA felt a need to defend its business - characterizing its longstanding strategy as enduring and defensible - given the ongoing conversation in healthcare related to health system disruption.
- “Beyond inflation and high labor costs, health systems are struggling because competitors—ranging from vertically integrated payers to PE-backed physician groups—are effectively stripping away profitable services and moving them to lower-cost care sites. The tandem forces of technological advancement, policy changes, and capital investment have unlocked the ability of disruptors to enter market segments once considered safely within health system control.”
Despite the above rhetoric, HCA seems insulated, and there’s a reason for that. HCA is objectively an incredible, cash-flowing business that has survived and thrived through multiple take-privates, significant healthcare reforms.
How?
They are thoughtful about the markets they enter and exit and the population characteristics present in each. Their hospital and ambulatory footprint is massive. HCA market demographics generally are faster growing from a population standpoint, have higher income, and are stronger jobs markets.
Neuro & Stroke Centers
Blake takes a look at this topic as it relates to outpatient migration:
- This quote in context is hilarious, as HCA seems almost exasperated by the constant ‘shift to outpatient’ narrative they’re having to battle: “Sam referenced the diversity of our portfolio. We’re not dependent on any 1 single service line for greater than 14% of our inpatient hospital net revenue. This mitigates risk, risk from having new drugs to market that may prolong a patient getting treatment or that shift from inpatient to outpatient we’ve been talking about for 10 years. This contribution margin, as you might expect, is higher than our average contribution margin for these complex patients. One reason we go for that.”On recruitment away from academic medical centers: In the old days, those physicians would probably have been attracted to an academic medical center. We’re faster, we’re more nimble. We give them voice. We are less bureaucratic and physicians love that. These academic centers without our scale are at a competitive disadvantage. And so this growth in CMI has generated net positive growth on our revenue. The first example I want to give you is our neuro. In 2016, we took a very deliberate approach to building the infrastructure by building out these comprehensive stroke centers. These high acuity patients often require surgery or intervention as that first video you watched. This impacted both our case mix and our market share. We added 10,000 incremental admissions over this time period, 121% growth in our stroke surgeries.
"Investment in higher acuity service lines."
Blake goes on to examine:
40% of HCA revenue comes from high acuity services across specialties like cardiology, oncology, and orthopedics. Given aging populations and more advanced diseases, we’re going to see that acuity and case mix continue to grow. Makes sense that you’d want to continue to target higher acuity stuff as HCA given that outpatient migration is capturing market share in lower acuity services within ASCs and OBLs. This strategy more effectively insulates HCA from that threat, but HCA still holds execution risk with its ability to recruit highly sought after subspecialists to perform higher acuity services in its hospitals.
This quote in context is hilarious, as HCA seems almost exasperated by the constant ‘shift to outpatient’ narrative they’re having to battle:
- “Sam referenced the diversity of our portfolio. We're not dependent on any 1 single service line for greater than 14% of our inpatient hospital net revenue. This mitigates risk, risk from having new drugs to market that may prolong a patient getting treatment or that shift from inpatient to outpatient we've been talking about for 10 years. This contribution margin, as you might expect, is higher than our average contribution margin for these complex patients. One reason we go for that.”
"HCA is fine with physician independence"
Blake pulled this quote from HCA's investor day:
In order to attract physicians, we've developed a value proposition. As I mentioned, a number of our physicians are independent. So generally, they are selecting where they admit their patients and where they choose to practice. The key elements of a value proposition that we've identified are giving physicians voice, creating capacity, both physical capacity, but also efficiency in their practices, helping them grow and then wrapping it around exceptional clinical capabilities. We strive to give physicians voice to ensure that they are heard. Jon talked about the physician relations representatives that are out in the field, interacting with our medical staff, understanding what we do well, so we can do more of it, understanding where the challenges are in our health system so that we can carry that back to our operators, and we can continuously improve.
On recruitment away from academic medical centers:
Blake pulled these quotes:
In the old days, those physicians would probably have been attracted to an academic medical center. We're faster, we're more nimble. We give them voice. We are less bureaucratic and physicians love that. These academic centers without our scale are at a competitive disadvantage. And so this growth in CMI has generated net positive growth on our revenue. The first example I want to give you is our neuro. In 2016, we took a very deliberate approach to building the infrastructure by building out these comprehensive stroke centers. These high acuity patients often require surgery or intervention as that first video you watched. This impacted both our case mix and our market share. We added 10,000 incremental admissions over this time period, 121% growth in our stroke surgeries.
Click here to subscribe to Hospitalogy.
|
Congress
4. U.S. House Passed Site Neutral Payment Package Before Leaving for the Year
| |
The U.S. House passed a new site neutral payment concept bill that would create a site-neutral payment policy for hospital-administered drugs in the hospital setting.
Click here for an explanation from STAT News. Click here for an explanation from Axios.
As you read in the article about Medicare physician payment cuts, 2024 legislation that would lead to significant long-term health policy changes is unlikely in an election year. As a result, odds are against the legislation also clearing the U.S. Senate in 2024.
Site Neutral Payments: A Big Issue in State Legislatures & Washington
The site neutral payment policy issue continues to be a major issue in Washington, especially as a tool to address consolidation. State legislatures are beginning to look at the concept.
In the 2023 Texas Legislature, the site neutral payment issue posed as one of the greatest public policy challenges in recent memory for Texas hospitals. The Texas Legislature eventually walked away from the issue in 2023.
The American Hospital Association argued that facility fees for services that can be found in physician offices and ASC settings are necessary to offset hospital overhead.
The issue will continue to be debated in Washington in 2024.
| |
Industry
5. What We're Reading: New Federal Government Merger Guidance, AMA's Promotion of Physician-Led Hospitals & More
| |
AMA Council on Medical Service Offers Additional AMA Support for Physician-Led Hospitals
The AMA's Report of the Council on Medical Service represented the organization's latest support for physician-led hospitals:
Longstanding AMA policy supports the repeal of the ban on POHs, and the AMA has been actively advocating for the repeal as recently as 2023. The AMA’s June 2023 letter of support for the Patient Access to Higher Quality Care Act of 2023 underscores that POHs have been shown to provide high-quality care to the patients they serve. The Council believes that not only does limiting the viability of the POHs reduce access to quality medical care, but it also reduces competition in hospital markets to the detriment of the communities these hospitals serve.
One of the strongest opponents of POHs is the American Hospital Association (AHA). In a comment letter to Congress on H.R. 977/S.470, the AHA claims that POHs “provide limited or no emergency services, relying instead on publicly funded 911 services when their patients need emergency care.” However, the majority of POHs are generally equipped with several hundred beds and large emergency departments similar to community hospitals. A report by CMS in 2005 found that physician-owned cardiac hospitals resembled full-service hospitals with emergency departments, whereas orthopedic hospitals and general surgical specialty hospitals more closely resemble Ambulatory Surgery Centers (ASCs) which focus on outpatient services or cases with a reasonable expectation of limited hospitalizations. For example, POHs with specialty care, like cardiac care, closely resemble full-service hospitals with emergency departments, while POHs that specialize in orthopedic care closely resemble other outpatient facilities or ASCs. The differences are driven by services provided to patients and are not drive by the ownership structure of the hospital.
Additionally, in their comment letter, the AHA claims that “physician self-referral also leads to greater utilization of services and higher costs.” The Council believes that this is also a misrepresentation. CMS studied referral patterns associated with specialty hospitals among physician owners relative to their peers and ultimately stated: “We are unable to conclude that referrals were driven primarily based on incentives for financial gain.” Several studies looking at the effect of hospital ownership on health care utilization have concluded that physician ownership does not lead to an increased volume of surgeries being performed, suggesting that any evidence of increased utilization is at best mixed.
Finally, the AHA claims that “physician-owned hospitals tend to cherry-pick the most profitable patients, jeopardizing communities’ access to full-service care.” To the contrary, evidence indicates that physician-owned hospitals do not “cherry-pick” patients. For example, CMS studied referral patterns associated with specialty hospitals among physician owners relative to their peers and were unable to conclude that referrals were driven primarily based on incentives for financial gain. Importantly, new economic research also finds strong evidence against “cherry-picking” in POHs.
Federal Government Released 2023 Merger Guidelines
The U.S. Department of Justice and Federal Trade Commission released the 2023 merger guidelines on December 18. Click here to view the press release.
The guidelines represent President Biden's Executive Order on Promoting Competition in the American Economy (July 2021), which states that:
…To address the consolidation of industry in many markets across the economy, as described in section 1 of this order, the Attorney General and the Chair of the FTC are encouraged to review the horizontal and vertical merger guidelines and consider whether to revise those guidelines.
Per the press release:
Like the prior horizontal and vertical merger guidelines they replace, the 2023 Merger Guidelines are not themselves legally binding, but provide transparency into the Agencies’ decision-making process.
The 2023 Merger Guidelines do not predetermine enforcement action by the agencies. Although the Merger Guidelines identify the factors and frameworks the agencies consider when investigating mergers, the agencies’ enforcement decisions will necessarily depend on the facts in any case and will continue to require prosecutorial discretion and judgment.
OIG Opinion:
Employed Physicians in Multi-Specialty Practices That Tie Profits to ASCs
Click here to view the OIG's October 10, 2023, advisory opinion. Reply to this e-mail for a deeper analysis.
Private Equity: The Federal Government's Recent Activity
The Centers for Medicare and Medicaid Services (CMS) published a final rule related to the federal government's new requirement for nursing homes to disclose privatey equity and REIT ownership.
The Freakonomics podcast recently took a look at private equity ownership in nursing homes.
The U.S. Federal Trade Commission asked physicians for feedback regarding their experiences with private equity.
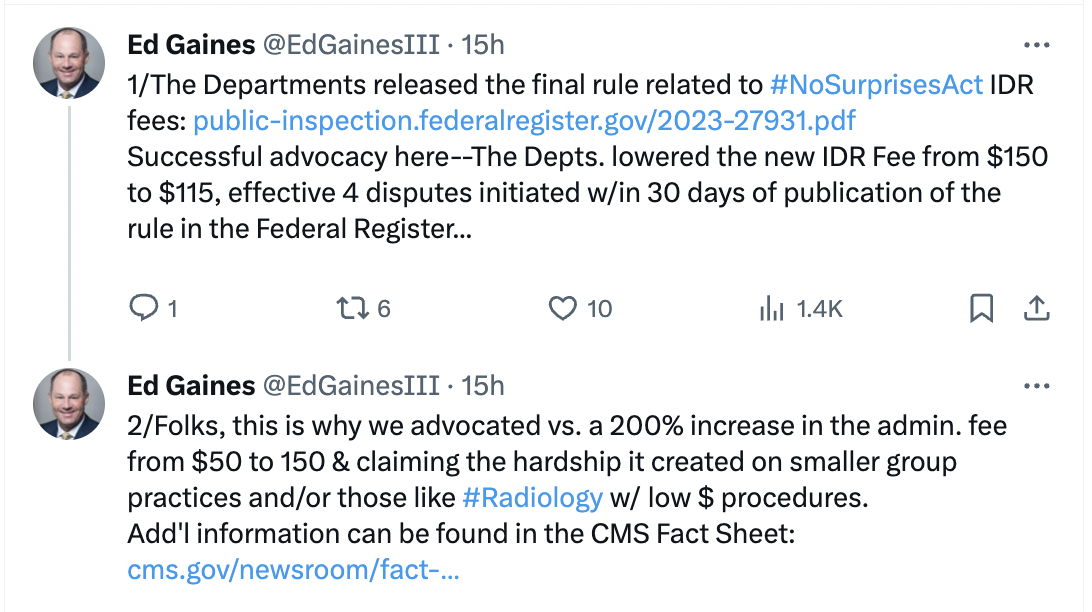
New Independent Dispute Resolution Fee Rule
CMS released the new fees related to the IDR on December 18. Of note:
- An administrative fee of $115 per party has been established.
- An IDR entity fee range of $200-$840 for single determinations.
- An IDR entity range of $268-$1,173 for batched determinations.
The Departments further indicated that this final rule:
- Retains the process for certified IDR entities to set their fees once per calendar year within the ranges last set forth in rulemaking or to request written approval to set their fees outside of the set ranges; and
- Allows certified IDR entities to request to update their certified IDR entity fees one additional time per calendar year, subject to the Departments’ approval.
Ed Gaines, one of PHA's 2023 Leadership Summit's keynote speakers, provided his reaction on X yesterday.
| | |
Physician-Led Hospitals | Value Care | New Models for Expansion
6. PHA's Summit Recap Webinar Replay Available: A Look at the Latest Legal Issues With Amber Walsh & Her Team
| | |
In case you missed it, this week's Leadership Summit recap, which examined the latest legal issues facing PHA members, is now available.
Reply to this email for a copy of the webinar, which featured PHA's president, Joseph Alhadeff, MD, PHA's legal counsel, Amber Walsh, and her colleague, Kristen Woodrum.
The zoom took a look at the latest legal issues facing physician-led hospitals, value-based care and innovative ways to create new physician-led hospitals.
| | |
Congress
It's Time for Patients & Surgeons to Engage Congress: PHA's My Care in My Community Campaign
| |
It's time for Congress to hear from their most important constituents - patients and physicians - about the importance of expanding physician-led hospitals.
PHA made it easy for PHA members to encourage their patients, surgeons and employees to engage Congress through PHA's My Care in My Community grassroots campaign.
Click here to get started. And please share it with your patients and staff.
| | |
September 21-23, 2024 | Florida
The Ritz-Carlton Naples:
PHA's 2024 Leadership Summit
| | |
Save the date for PHA's 2024 Leadership Summit September 21-23 at the Ritz-Carlton in Naples, Florida.
The new format will begin after lunch on Saturday, September 21 and conclude before lunch on Monday, September 23.
PHA will announce the preliminary speakers later this month. Registration will begin in mid-January.
| | PHA's 2023 Title Sponsors: | | PHA's 2023 Executive Sponsors: | | PHA's 2023 Premier Partners: | | |
Stacie Monroe
Physician-Led Healthcare for America
Stacie@physicianled.us | 419.250.5873
| |
Physician-Led Healthcare for America Website
| | | | | |